
THINGS HAVE BEEN PRETTY BAD FOR A WHILE...Scroll down to a section in blue below to read one doctor's experience. Thousands are doctors around the country have their hands tied by their hospital administrators. General public is largely unaware or non-medical professionals impact patient care. Doctors have been facing and reluctantly complying with growing impositions from a wide range of sources. Here are some examples: - insurance companies limiting the ability of doctors to prescribe medications that would be ideal for an individual patient and many insurance companies pay doctors laughable amounts for the work they do (trust me on that) - medical coding system (each diagnosis and procedure has an assigned number, and many of the diagnostic code names make very little clinical sense - electronic medical record systems (the vast majority of which have completely altered the normal physician workflow and how we gather, process and share information with each other) - legal field (there is always a possibility of being sewed even if you did ABSOLUTELY NOTHING wrong) - hospital systems that work their doctors to death (if you don't know many doctors, that's because they are probably always at work and only socialize at the expense of sleep or some other vital necessity) - ridiculous board exams, which in no way correlate with whether or not a doctor is knowledgeable and does an amazing job at caring for his or her patients (these exams take many weeks of study of random information we rarely use in real life, and take us away from patient care; not to mention, most of them are over $1,000 each (+ a few thousand for a prep course + $1,000 if you have to retake it) and have to be taken every 5-10 years. For at least a few decades, doctors have been working on fumes (most work 60+ hours/week, many even more - I personally have regularly worked 100+ hours per week). We do not get enough sleep. We often don't have time to eat. I can't tell you how many times nursing staff would sneak in a plate of food in front of me while I was documenting patients histories patient charts, because otherwise I would not eat at all in the 9+ hour shift. I simply did not have time (trust me it was not by choice!). I can't tell you how often, as I was leaving work, I would realize that I have not had time to go to the bathroom. At all, in a 10 hour day! All of this is so wrong and unhealthy, but for many of us, it's our reality. Sadly, I am not an exception... Many doctors around the country will tell you similar stories. The sad part is that things have been getting worse and worse every year. It's true that we now have work hour limitations have been placed onto resident and fellow physicians (doctors in their first years of working as physicians - no more than 80 hours/week and 24 hr/day of patient care [not including charting, lectures, etc, etc]. So yes, resident and fellow physicians do work a little bit less now than before, but as soon as you are done with residency or fellowship, this rule no longer applies. So yes, it's madness. Going back to my point. Things are getting worse every year. Doctors are too busy taking care of patients, simply don't have time to fight the overwhelming force of external forces that ultimately impact how we care for our patients. Thus far, we've been able to adjust, each of us figuring out was to "work around" the system in order to deliver the best possible care to our patients. Today, these major external forces have surpassed every boundary. Today, during this tragic pandemic, doctors are literally being forced to do the wrong thing! Many are threatened by being fired if they don't comply. I literally see hundreds of horrifying posts from doctors in private Facebook groups every day. The vast majority can't do ANYTHING to fight this! Doctors are in a horrible position because they have an obligation to their patients, and even when hospital administrators do not provide doctors with proper masks, doctors are still going in because they can't let their patients die! It is wrong for non-medical professionals to dictate how doctors should do their job. You want doctors, not administrators making medical decisions. It is obvious. It is common sense. And yet, now more than ever, we have reached an unprecedented level of admitrators controlling patient care. Please read one doctor's story below. Please share it. WHAT'S HAPPENING NOW. A DOCTOR'S EXPERIENCE."Mostly venting. And physically sad/angry/upset at my hospital’s response to COVID. Here’s my two specific examples. (I’m FM) [Family Medicine Doctor] 1. Radiology is being told by administration that they can’t use the word COVID in their reports. It’s “scaring staff”. So they can’t say in a CXR [Chest X-ray] report “patchy bilateral infiltrates consistent with COVID,”. They just have to stop at “patchy bilateral infiltrates.” Same for CT scans, which to my knowledge, can be nearly diagnostic of COVID. We do not do this for other diagnoses. We would not hesitate on a mammogram to describe a breast lesions and say “highly suspicious for malignancy” or describe the pancreas on CT and say “consistent with pancreatitis.” Also, if/when our patients get transferred to outside hospitals, and only the imaging report goes, not the images, the receiving doctors will need to read between the lines. 2. There are two small hospital systems in my entire county. On Friday, the media reported that my county had the first positive confirmed case. The two hospitals released a joint statement saying that The case was not at either one of the hospitals. This confused me. Then my Hospital went out of his way to make another statement on Saturday again reiterating that the case was not at our hospital. However, I know that my hospital like we has four or five pending cases. I’m angry that my hospital system is either trying to deceive the public, downplay the situation, or make it look like we are still a safe place to come because COVID “is not here”. Or maybe there’s another tactic that I don’t understand. But I don’t like it." Family Practice physician (Publishing anonymously per doctor's request) Administrators can’t tell us how to do our jobs. If the radiologists stop using the phrase “consistent with...” it may potentially affect clinical decisions that other doctors will be making (those who provide direct patient care based on on the the radiology reports). Which means, if radiologists comply with what hospital administration demands of them, it may cost people’s lives. Our primary obligation as doctors is to our patients, we all gave a “do not harm” oath. This obligation is much stronger than any other duty we have to our employers, or others who impede good patient care. We have never in our careers had to experience such a discrepancy between what we are told to do and what is right. On top of that, doctors who are trying to do the right thing, are being threatened with being fired. Here is the thing. It's not that doctors are afraid to lose their jobs. No, they are not thinking about themselves. Doctors are concerned about patients and who will take care of them if the doctors are not there. They do not want to be forced to abandon their patients because the hospital administration is making wrong decisions. That's why doctors find all this to be so overwhelming. They are stuck between a rock and a hard place. PLEASE HELP!As you read these words, I hope you can understand the tough position the doctors are in right now.
If doctors don't have the right masks or other protective equipment, they should not be treating patients potentially exposing them to the virus. Please refuse to be seen by a doctor (or any healthcare provider) who is not properly protected. Doctors should not be told by their hospital administrators how to their job. Doctors should not be risking their jobs if they are doing what's right. Don't let some bureaucrat decide your fate and the fate of your doctor. Please help your doctors. They are there to help you. They put their lives at risk to help save yours. Ask your doctor what you can do to help. If you see something like this happening in your community, please talk to the press! The doctors can't help themselves right now. They need you to help them take care of you the right way. Please share! People have to know!
0 Comments
I spend hours going through all the available data on SARS-CoV-2, the virus that is causing current pandemic, I also communicate daily with front-line physicians and experts, who understand this disease better than all of us. Many of these frontline physicians are not able to share their experiences publicly out of the fear of retaliation from their hospitals' administration and also out of concern about the reaction of the public. In the end, this important information needs to be shared so that the people can make educated decisions about how to protect themselves and how to help protect their healthcare providers: Below is a letter from one of the doctors, whom I consider to be an expert : A LETTER FROM AN EXPERT"I have debated whether to post about my suspicions regarding airborne transmission of SARS-CoV-2 and COVID-19, whether I’d be causing unnecessary panic over something we can’t do a whole lot about. I think it’s time.
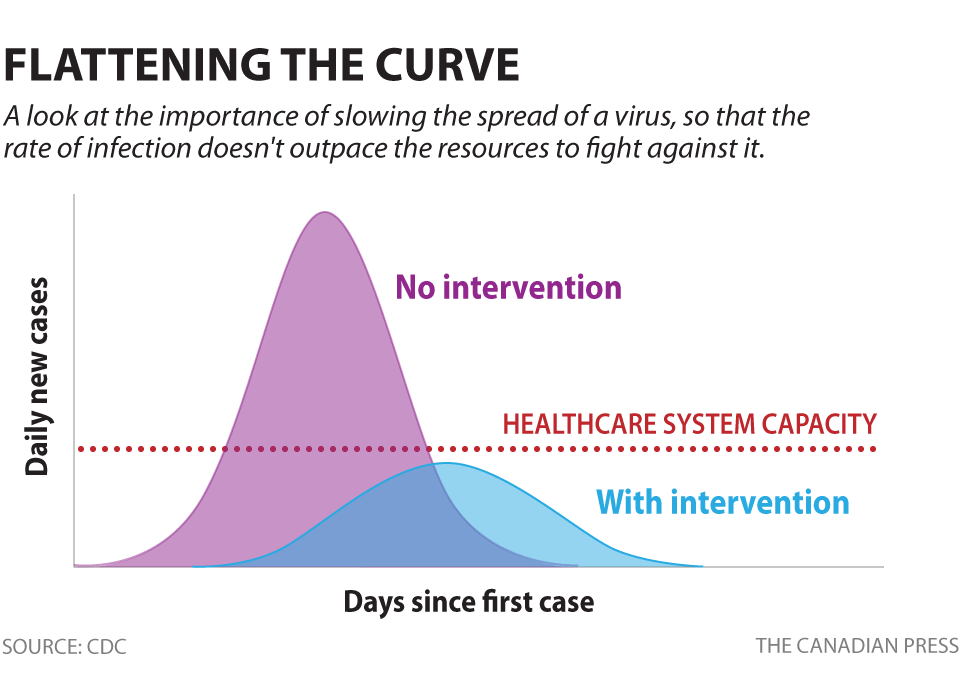
There is much I can’t say in public that’s scaring the crap out of me and keeping me up all night. Those of you who know me well, know that I research exhaustively and am very logical and data driven. The data is bad. I am the lead author of several publications on aerosol deposition in the airway. So when I talk about aerosol inhalation, I have more in depth understanding of this than most physicians. Not all—some know a lot more than I do. But most. Airborne vs droplet precautions are archaic. Airborne precautions require healthcare workers to don previously fit tested N95 masks or PAPRs (powered air purifying respirators), in addition to eye protection, gown, and gloves. Fit testing, which must be done before a healthcare worker can safely use N95 masks, ensures no air can be inhaled through gaps between the wearer’s skin and the edge of the mask. This is critical. Droplet precautions require a regular surgical mask, gown, eye protection, and gloves. Airborne transmission relates to an infectious agent’s ability to infect others at a significant distance through aerosols. Aerosols are small particles of potentially infectious material generated by coughs and sneezes. Aerosols remain suspended in the air for some time. They don’t immediately fall and land on surfaces like the larger particles, droplets, do. Aerosols suspended in the air can infect others in close proximity, even if a disease is not classified as “airborne.” We know the coughs of a healthy person generate aerosols. not just droplets. We know viral infection (specifically influenza) can increase the percentage of small aerosols generated by a cough. We know small aerosols penetrate deep into the lungs. This is thought to be a mechanism by which influenza enhances its transmission from host to host. SARS-CoV-2 might be able to do the same. We just don’t know yet. Small aerosols <= 5 micrometers reach the lung alveoli when inhaled. That means the deepest lung tissue, where gas exchange occurs. SARS-CoV-2 remains viable in the air for hours, at a minimum, when aerosolized in vitro. And it is postulated that the method of transmission on cruise ships may include true airborne, through the ventilation systems. A regular surgical mask doesn’t protect the wearer against aerosols. It only helps to protect against droplets, for those in close proximity to expelled airway secretions. It also helps to keep the wearer’s own droplets in, to protect others and to maintain sterility. But it won’t stop anyone from inhaling aerosols Asymptomatic and mildly symptomatic people are contagious, as are their coughs. They probably don’t know they have COVID-19, and probably aren’t socially isolating. The cases we know about are just the tip of the iceberg. You’re probably breathing the virus in from someone’s cough, even if you don’t know it, as well as contracting it through contact with droplets, contaminated surfaces, and possibly the fecal-oral route. If people don’t start DRASTICALLY socially isolating, we have no hope of flattening the curve. HEALTHCARE WORKERS NEED N95 OR PAPR DEVICES NOT TO DIE. Please help by contacting your local, state, and national representatives, as well as philanthropists, to make them aware of the urgency of our need. And please, please stay home and stay away from others. Your life, the lives of those in close proximity to you, the lives of those you meet in passing, the lives of healthcare workers who may treat you, and their families’ lives, depend on it. Thank you." Physician, FL Anonymity preserved per doctor's request As of 03/20/2020 we still don't know enough about Coronavirus transmission. MY VIEWFrom my personal extensive analysis of the available data (references are available on this page) it is clear to me that the virus can be transmitted in the following way:
Additionally, it appears that SARS-CoV-2 (the Coronavirus responsible for this pandemic)
EXPERT VIEWCheck out a litter from an expert on the subject of transmission. It is really eye-opening... CLICK HERE to view the blog post with the letter. Please take the time to read the letter. It is important. Please share it as well. WHAT IT MEANS FOR YOUBe conscientious about your own hygiene and take active measures to protect yourself and others:
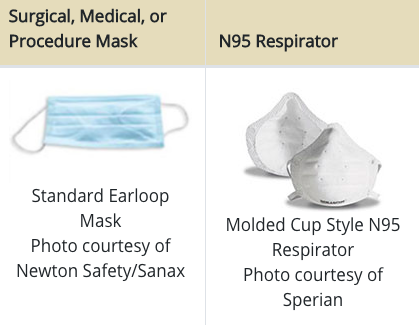
I know this is a lot to take in, but it will save lives. I am sorry if the information keeps changing all the time! I will do my best to continue keeping you updated. With love and care, Dr. Maria Danilychev, MD www.danilychev.com P.S.: Below are some images that may help makes sense of all the PPE (personal protective equipment) PERSONAL PROTECTIVE EQUIPMENTWhen around people outside of your home:To protect yourself from droplets in case some coughs or sneezes on you (and to protect the others from your own accidental cough or sneeze), you can use a scarf if you are not sick and a mask if you are (PS: please don't go in public if you are sick): PPE for healthcare workers
If you are sick at the hospital with a respiratory infection, you want all your doctors and care providers to look like the BEST photo above in the ideal case scenario.
Which masks are currently provided to healthcare workers? Very few get PAPRs, many do not have access to N95s, some healthcare workers don't even have enough regular masks, any many are instructed by their hospital administrators to wear suboptimal protective equipment to avoid "scaring" the public. Honestly, I would be more scared of a doctor who is unprotected and may be passing germs around, then the one who is fully "suited up". Please do whatever you can to help! You don't want people in the front lines to start getting sick and dying. Who is going to help the rest of the people? Physicians are notorious for being really bad at advocating for themselves. I've been asking everyone how is not adequately protected by their healthcare organization to speak up, but very few people are doing it. It will take a public outcry to for this horrible situation to change. I am doing everything I can to increase public awareness of this issue which is largely hidden from the public eye and which is not being adequately addressed. Please spread the word! Please find ways to contribute PPE to healthcare workers near you! This is a quote from a doctor from Rockport, Maine. This physician's viral post in a Facebook Group for medical professionals fighting COVID-19 has received hundreds of "ME TOO!" replies from around the country within hours. The doctor has agreed for me to share her outcry with you, requesting to be anonymous to avoid potential retaliation from her hospital administration. It may be one person's voice but it saying what's on the minds of so many! This is real. Please read. "Warning. Vent: I am starting to feel so confused. Too many questions, too little evidence based data, too many rapidly changing “guidance”, too many hypothetical answers. No PPE*, horrid non existent access to testing. We give and sacrifice so much for this job, this calling, this privilege of being a doctor, a job we love and now.... we are left out here vulnerable and abandoned. I just can’t wrap my head around it. So many of us exposed, maybe exposed, likely exposed. Our kids sick, family members sick, our patients sick and we have NO GD ANSWERS. So if my kid has a 104 fever what do I do? Go to the hospital, don’t go to the hospital? Ask for a test? Get a flu test? Yes you can be coinfected, but maybe not. Only this age or that age. No freakin actual facts. Good luck, sorry doc. You don’t meet the “criteria”. Your kid doesn’t meet “criteria” your patient doesn’t meet “criteria”. The magic fvcking criteria made up by people NOT on the front lines. So what do you do? Stay home, go in, possibly expose more people? Stay home for 3 days, 10 days, 14 days? Repeat test, oh wait no test done. So don’t repeat test. Wear a respirator, wait no surgical mask ok. It’s probably airborne and probably droplet. Use an N95 until you have the results of the test you can’t order. Really?!?!WTGDF !? It’s like a bad Vietnam War movie. The guy 1000 miles away from the gunshots is making all the decisions and he doesn’t really care if you live or die. This can’t be the reality. I feel like I’m losing my mind. For $10 I’d put my family in the car, drive off into the woods and camp for the next 6 months. It’s all too much. Someone has to do something! Meanwhile people across the country- some my family and friends! Out in bars, out having fun without a care in the world. Not a shred of reality. And we will be resuscitating them and passing it- this amorphous unknown unpredictable motherfvcker of a virus to ourselves and our families. Why?!! I’m just totally lost." * PPE - Personal Protective Equipment (like facemasks, etc.) DOCTORS' HANDS ARE TIEDAlthough some hospitals are doing an excellent job with COVID-19 reponse, it appears that many doctors are forced to work without proper protective equipment. Many doctors feel that their hands are tied by hospital administrators. Here is what this doctor had to say about the situation many physicians are facing. (Reposting with the doctor's permission): "When exactly did physicians lose control of our profession?😢 I’ve read all the posts in this group, and am sensing such powerlessness and despair: story after story by my physician colleagues all across the country, of “ADMIN” * mandating things during this COVID19 crisis that we as physicians know are unethical and unsafe. They sit in their safe offices telling us that even though we have inadequate PPE** , we must make do and continue to work, reuse PPE and ask permission to access N95 masks*** that they’ve locked away. They’re refusing to “allow” us to cancel non-urgent routine appointments and surgeries -we have to wait for admin to decide. They’re refusing to “allow us” to test patients we know should be tested. They’re forbidding us from publicly posting about the crisis because we are “inciting panic.” They’re threatening our jobs if we don’t comply. We are afraid to speak out because we don’t want to lose our jobs. We’re afraid to refuse to see patients without adequate PPE, both because of “admin” and a misguided sense of duty. Every one of us that are working without PPE are at high risk of infection, and will become super-spreaders. We’ll be passing it along to subsequent patients during our asymptomatic period, and bringing it home to our families, before we then become infected patients ourselves. Won’t we end up infecting more people overall than if we refused upfront to see pts without adequate PPE? We have no union, most of us are employees following the direction of people with half the education and intelligence than us. They’re the kings sitting on horses directing us lowly soldiers at the front line to charge, without swords and shields. When did we become so powerless? And when this crisis is over, is anything going to change? Sorry for the rant and I actually don’t have the answers, just felt the need to vocalize what so many are feeling. God protect us all 🙏🏽 (ETA to be fair: I must say on a personal note that my organization has been overall very responsive to the concerns of its PCPs****, received our constructive feedback/suggestions and started instituting changes within the last week like 90% telemedicine, remote work for high risk PCPS...mainly because it is PHYSICIAN led. This is also why we need to #takebackmedicine.)" * "ADMIN" - referring to hospital administration in this case
** PPE - personal protective equipment, such as face masks *** N95 masks - the masks healthcare workers should be using to be protected from Coronavirus **** PCP - primary care physician/provider "Dear friends. My fellow humans. Please share.
I don’t know what to do. I literally want to cry right now because so many people I know are taking what’s happening with coronavirus too lightly. We are on the brink of a preventable global catastrophe due to this pandemic. We only have a few days left to help the situation and in one very simple way. PLEASE STAY HOME! Yes, it’s that simple. Don’t go anywhere for a few weeks unless it is necessary for your survival. I know it sounds extreme, but there are lots of asymptomatic carriers in the community who haven’t been diagnosed with COVID-19 yet and who are unknowingly spreading the disease. Every time you leave your home, not only you are exposing yourself, you are potentially exposing EVERYONE you come in contact with for up to 4 weeks of getting the virus! (It’s less than 2 weeks in 99% of cases, but there is that 1% that’s also very real.) Even if your own symptoms are mild to none, you can infect others! By leaving your home you could unwillingly contribute to someone’s demise. I know you don’t want that. It doesn’t matter if you are young and healthy. If you are around other people, you may still get the virus which could be deadly to you or to someone you care about. I’d like to make a parallel. It might sound shocking perhaps. I want to compare us leaving our homes right now to drunk driving. We can all agree that drunk driving puts people’s lives in danger. Imagine if every time you left your home you were at risk of returning completely intoxicated and accidentally hurting someone close to you. And that each time you left home, it could lead to several new drunk drivers who could kill someone? And that each of those people would create their own “set” of deadly drunk drivers and so on, like a domino effect? Can you imagine? This is exactly what this is like, but worse! Experts in pandemics have extremely grim predictions of what will happen with COVID-19 and with the devastation that it will bring to the world. Millions will die, and it’s not science fiction. It’s reality. Please. I am begging you. Try to hear what I am trying to say. Let’s make those predictions wrong by doing what no scientist could predict! By being kind, thoughtful, and responsible human beings - by staying home. Every single one of us! In a few weeks, when we start seeing the aftermath of our careless decisions, it will be too late! Don’t wait until a mandatory quarantine is instituted. Stay home now! By doing this you will be preventing the virus from spreading, and will help save hundreds of thousands of lives! I don’t know how to help people understand just how critical this is, and how important it is for it to happen TODAY, NOW! I don’t know if you can hear me, but I hope you do. Please share. If it saves even just one life, it’s worth it. Writing to humanity in desperation on March 15th, 2020 from San Diego, California. With love and gratitude, Dr. Maria Danilychev, MD"
COVID-19 GRAPHSADDRESSING VENTILATOR SHORTAGES
Off-label use of one ventilator to save multiple lives.
USEFUL LINKS FOR HEALTHCARE PROFESSIONALS
THIS SECTION IS CURRENTLY UNDER CONSTRUCTION - ADDITIONAL LINKS TO BE ADDED
MAP - Coronavirus interactive map
WHO - online training CDC - for healthcare professionals Stanford coronavirus study - please share CORONAVIRUS RESEARCH
THIS SECTION IS CURRENTLY UNDER CONSTRUCTION - ADDITIONAL LINKS TO BE ADDED
03/14/2020. QUOTING JOHN DONATI.Quoting a friend of mine who lives in the Northern part of Italy (see original text in blue below): ENGLISH TRANSLATION [by Dr. Danilychev] [03:13, 3/14/2020] John Donati: "in Italy 50% of the people who are positive for the virus and manifest the symptoms DO NOT have the need for a hospitalization. They stay hoe, usually have symptoms of light/moderate intensity also like the normal flu and get better in one week. 40% need to be hospitalized for two - three weeks. 10% need ICU [intensive care unit] care. 3-4% of the patients do not survive (at times even the young patients and in good health). The big issues is that the increasing number of people who are sick AT THE SAME TIME. In Italy, in 2 weeks the number of [ICU hospital] beds and [ventilators - ICU artificial breathing machines] has tripled and the number of healthcare workers of all kinds has increased to several thousand (over 4,000 [in some regions]) to the point of retired doctors being asked to work. All of this also means that ANY OTHER TYPE OF MEDICAL TREATMENT NOT CONNECTED TO COVID19 and that's not urgent is postponed until a later date (which means when the situation is going to be back almost to normal). [03:16, 3/14/2020] John Donati: "Therefore, the biggest problem remains that of containment of the contagion as much as possible. Otherwise, we'll arrive at a point that the hospitals will not longer be able to treat patients, both those affected by covid 19 and those affected by any other condition." [03:13, 3/14/2020] John Donati: "in Italia il 50% delle persone che sono positive al virus e manifestano i sintomi NON hanno bisogno di cure ospedaliere. Stanno a casa, di solito hanno sintomi lievi/di media intensità quasi come una normale influenza e solitamente guariscono in una settimana. Il 40% hanno bisogno di cure ospedaliere fino a 2/3 settimane. Il 10% ha bisogno di cure intensive. Il 3-4% dei pazienti non sopravvive (a volte anche pazienti giovani, sani e in forze). Il problema grande è il numero elevato di persone malate CONTEMPORANEAMENTE. L'Italia in 2 settimane sta triplicando il numero di posti letto e di macchinari per la terapia intensiva e ha aumentato di qualche migliaia (oltre 4.000) il personale sanitario di ogni tipo, arrivando persino a richiamare in servizio i medici in pensione (retirement). Tutto ciò significa anche che QUALSIASI ALTRO TIPO DI CURA MEDICA non legata al COVID19 e non strettamente necessaria è stata posticipata a data da destinarsi (which means when the situation is going to be back almost to normal)." [03:16, 3/14/2020] John Donati: "Quindi il problema più grande è e rimane quello di arginare il più possibile il contagio. Altrimenti si arriverà al punto che gli ospedali non saranno più in grado di curare i pazienti, sia quelli affetti da covid19 che quelli affetti da qualsiasi altra patologia." 03/14/2020. QUOTING SIMONA CORRA'.Quoting another friend of mine who lives in the Northern part of Italy (see original text in blue below, and some of my replies in black): [Simona Corrà]: "Here in Milan there are very few contagions at the moment but because all the activities have been stopped: museums, cinemas, schools ... even churches have been closed! The bad things that this virus is carrying are great irrational fear and racism. I really hope it will end soon." [Simona Corrà]: "Lombardia, my region, is the one with the most cases" 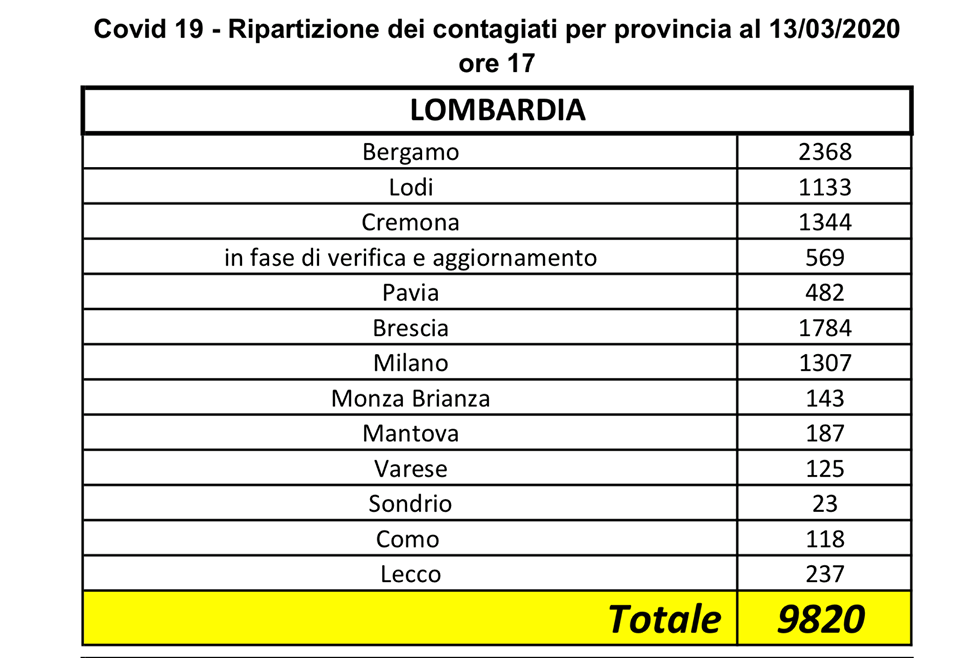 [Simona Corrà]: "We are fine, even my friends who live in Milan, but we are all closed at home. Only a family member can go out, and only for important reasons (such as going to buy food or going to the pharmacy)." [ Dr. Danilychev]: "It’s one of those things, people think “it’s over there, it will never happen here!” [Simona Corrà]: "Yes, it is true, it also happened here in Italy. It was thought to be a problem only in China and instead ... [Simona Corrà]: "also write something to make people understand the seriousness of the problem: people must not panic (among other things, stress lowers the immune system, right?) But people must prevent as much as possible, adopting all the hygiene systems basic and avoiding going to crowded places and, if the situation worsens, staying at home." 03/2020. QUOTING SIMONA CORRA'Quoting Simona Corrà: [Simona Corrà]: "[Dr.] Massimo Galli, infectious disease specialist at the Sacco hospital in Milan, declares, 'It is not a simple influence. If people think we are exaggerating, I would like to tell them to come and see what happens in our wards." Patients multiply so doctors and nurses work between 12 and 14 hours a day to exhaustion.'
[Simona Corrà]: "I am writing to you from Milan, the capital of the Lombardia, the Italian region with the most contagions of Coronavirus. The government has invited all Italians to stay at home, even if we are well, and to go outside only for necessary reasons, such as buying food or get the dog out. Until April 3, many activities must remain closed to avoid the spread of the new Coronavirus COVID-19: schools of all levels, gyms, shopping centers, hairdressers, cinemas, museums, offices whose employees can work from home and so on. It is no longer just a matter of respecting the simple health rules (like washing your hands, blowing your nose in a handkerchief, staying indoors if you have a fever). Cases of contagion must now be contained because all hospital intensive care are full, and doctors are forced to decide who should be treated before the others, even though they are all urgent cases. There is no need to panic, it is also scientifically proven that fear and stress lower the immune defenses that must be at the top right in this period! But it is important to give due importance to this global pandemic, since it is no longer a problem for China alone. If we respect the rules we are given, by doctors and the government, we will save many lives, not just ours. Here in Italy we say #IoRestoAcasa ("I'm staying at home") and #AndràTuttoBene ("Everything's gonna be all right") because we want to continue living in serenity, keeping fear away." |
AuthorDr. Maria Danilychev, M.D., is a San Diego based medical doctor with 20 years of experience and board-certified in Internal Medicine, Geriatrics, Hospice/Palliative Medicine, and as a Hospice Medical Director. Dr. Danilychev also conducts clinical trials and was one of the first responders during 9/11. ArchivesCategories
All
|






 RSS Feed
RSS Feed